
I have been told that this is easy to armchair quarterback the response. Woulda, coulda, shoulda are easy ways to look at an event and rationalize how you would have reacted. This analysis was simply taking the plan, the one that we developed for this situation, and laying out and looking at how we did. From a military perspective, it is an After Action Review. A little premature since we have not made it to Stage 6, but a draft until we do.
It’s something that nobody expected
President Donald J. Trump
Press Briefing
14 Mar 2020
Well except for President George W. Bush and President Barack Obama. In the early 2000s, I, with a host of other people, was given the task of providing input to President George W. Bush’s National Strategy for Pandemic Influenza. My part was tiny since my expertise was with the use of the Army National Guard to support the Department of Defense (DOD) during national disasters. None the less, I wrote and commented on thousands of pages of documents over months and months of workshops and tabletop exercises. The National Strategy was just that, a whole of government, multi-agency, across all states and territories. The strategy was a living document, and over the last fourteen years has been updated several times as recently as 2017.
To keep this post relevant I am going to update it as more information becomes available. As I add information I will keep it in the same text and formatting. however, if I plan on deleting or changing information I will strike through the text not to alter the initial post.
How have we done at executing the tasks within the implementation plan? How does the Plan Execution Metrix compare to our current timeline?
WHO Pase 1 and 2: The Inter-Pandemic Period (2009 to 30 Dec 2019)
During this time period, between pandemics, there are no new influenza virus subtypes that have been detected in humans. They are also closely monitoring animals that may pose a substantial risk of human disease. During the first two phases of the WHO Global Pandemic Plan, the Federal Government Response is at Stage 0.
WHO Phase 3: Pandemic Alert Period
17 November 2019 the Chinese government logged the first case of someone in China suffering from unknown pneumonia, later identified as COVID-19.
31 Dec 2019 China reported a cluster of cases of unknown pneumonia in Wuhan China.
Stage 1: Suspected Human Outbreak Overseas (WHO Phase 3):
5 Jan 2020 WHO published their first Disease Outbreak News; this should have been the early indicator. At this time, the US Federal Government Response plan is to be implemented at Stage 1.
HHS has an entire list of items that would have gone into plan. Whether or not these happened, I can’t say since I am not privy to that information. I am assuming that they did. Most of these tasks revolve around coordinating with WHO and deploying rapid response teams to assess the situation and identify requirements for successful containment if the human-to-human transmission was suspected or confirmed.
The one task that stands out is that HHS and DOD prepare for the logistical support for the deployment of stockpile material, including equipment, supplies, and personal. In short, DOD be ready to move ventilators and PPE to the FEMA region/state that is the most critical need. From a strategic communications perspective, our message to the international community was to “encourage nations and international organizations to engage in rapid, coordinated assessments… the states/local/tribal regions to review their pandemic plans…” (Homeland Security Council 2006). Our voice to the public was to reassure the public, explain confirmed facts, and direct them to trusted information.
Goals:
- Rapidly investigate and confirm or refute
- Coordination and logistical support
Actions:
- Initiate dialog with WHO
- Deploy rapid response teams
- Amplify lab-based and clinical surveillance to region
- Prepare to implement screening and/or travel restrictions from the affected area (Implemented on 29 Jan)
Policy Decisions
- Pre-positioning of US contribution to International stockpile assets
- Use of the pre-pandemic vaccine
The US public-facing response during Stage 1 was that the virus was a minor threat that was under control, and the risk to Americans was very low. President Trump’s comments to CNBC and at his rally in Michigan supported the communications goals for stage 1, whether coordinated or not.
Stage 2: Confirmed Human Outbreak Overseas (WHO Phase 4 or 5): 13 Jan 2020:
There was official confirmation of a case in Thailand, which was the first recorded outside of China. The international outbreak triggered WHO Phase 4. At that point, the objective was to contain the outbreak to the region and domestically active our health and medical response. International, the US would look to restrict travel to and from the region and as setup arrival screening at ports of entry.
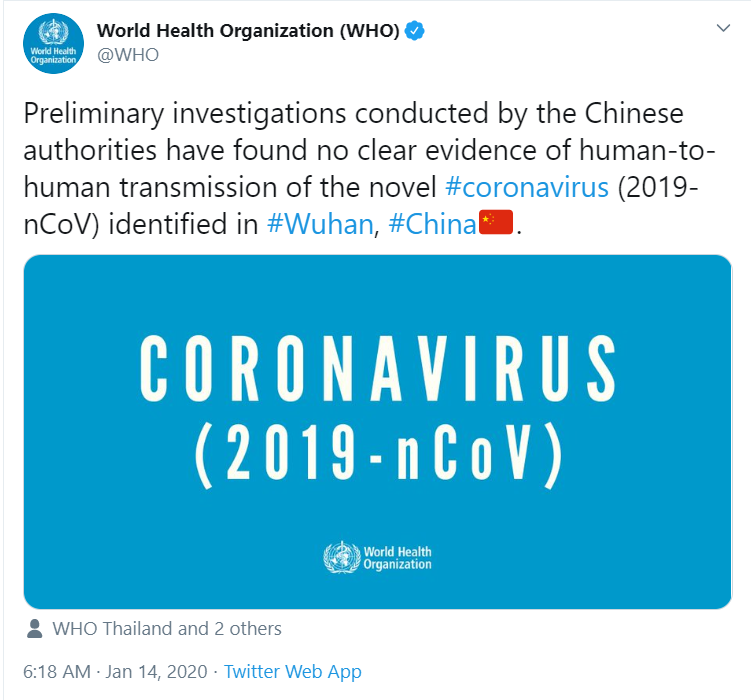
By 14 Jan, WHO’s technical lead for the response stated in a press conference that there may have been limited human-to-human transmission but quickly noted that this would not be surprising based on the WHO’s experience with SARS, MERS, and other respiratory pathogens.
However, there was a contradictory tweet by the WHO on the 14th
By mid-January, the first tests for 2019 novel coronavirus (2019-nCoV) were being developed. The WHO sent hundreds of thousands of tests to laboratories throughout the world.
On 22 Jan, the WHO mission to China issued a statement saying that there was evidence of human-to-human transmission.
Goals
- Contain outbreak and limit potential for spread
- Activate domestic medical response
Actions
- Declare Incident of National Significance
- Support Internationals deployment of countermeasures
- Implement layered screening measures; Activate domestic quarantine stations
- prepare to limit domestic ports of entry
- prepare to produce a monovalent vaccine
Policy decisions
- coordination to countermeasures for the affected region
- entry/exit screening criteria; Isolation / quarantine protocols
- revise prioritization an allocation of pandemic vaccine and antiviral medications
WHO Phase 5; Pandemic Period
Stage 3: Widespread Human Outbreaks in Multiple Locations (WHO Phase 6). 17 Jan 2020
On 17 Jan, the CDC started screening at three points of entry from passengers traveling in from Wuhan China. During Stage 3, the US goals were to delay the emergence of the pandemic in the US and North American populations and prepare our containment and response mechanisms. The steps for this would include limitations on international travel from the affected regions, prepare our national stockpiles for immediate distribution, develop and deploy diagnostic reagents to all Laboratory Response Network (LRN) Labs, active domestic emergency medical personal, and a have dozen other tasks. At this point, the WH should be prioritizing the efforts for domestic preparedness and response. From s communications effort, advise the public to prepare to reduce non-essential domestic travel once the epidemic REACHES the United States.
However, our public-facing message was President Trump stating that “we have it totally under control. It’s one person coming in from China”. This statement “coming in from China” verified that the first known case was on 20 Jan.
Goals
- Delay emergence in North America
- Ensure earliest warning of first case(s)
- Prepare domestic containment and response mechanisms
Actions
- Activate domestic emergency medical personnel plans
- maintain layered screening measures at borders
- deploy pre-pandemic vaccine and antiviral stockpiles
- real-time modeling; hospital-based surveillance
- prepare to implement surge plans at federal medical facilities
Policy decisions
- prioritize efforts for domestic preparedness and response
Stage 4: First Human Case in North America (WHO Phase 6) 20 Jan 2020
At this point, the US goals were to contain the first case, provide antiviral treatment and prevention, and implement the national response. Given that we did not have a rapid response test, treatment/therapy, and a vaccination, none of these were possible. Though several responses were possible.
Goals:
- Contain first cases in North America
- Antiviral treatment and prophylaxis
- Implement national response
Actions:
- Deploy our national stockpile to any domestic region with confirmed or suspected cases. (agreed to send some to Washington State on 3 Mar but should have had a “prepared to” supply by the 1 Feb)
- limit non-essential travel in affected areas and institute social distancing, yes this is in the 2006 plan, not something that we made up in 2020 (recommended in mid-Feb implemented on 11 Mar)
- Ensure that pandemic plans are activated across all levels of government and in all institutions.
- Activate surge plans fo Federal health care systems
- Amplify hospital-based surveillance in all communities (implemented early February)
Policy Decisions:
- Revision of prioritization and allocation scheme for pandemic vaccination
At this point, we should have some very vital messages to the public:
- Curtail non-essential travel
- Prepare for the implementation of community disease containment (closing schools, non-essential businesses, social distancing)
I think that there is an important note that needs to be added to this section. A 2017 study found that “75 percent of N95 respirators and 25 percent of face masks contained in the CDC’s Strategic National Stockpile (∼100 million products) were deployed for use in health care settings over the course of the 2009 H1N1 pandemic response.” In 2011, the Depart of Health and Human Services submitted a budget which included “$655 million, an increase of $59 million over FY 2010, for the Strategic National Stockpile to replace expiring products, support BioShield acquisitions, and fill gaps in the stockpile inventory.”
We recognized the need for replenishment of the stockpile and budgeted about a 10% increase that was rejected by the Republican House
Dr. Nicole Lurie
Assistant Secretary for Preparedness and Response
Department of Health and Human Services
I attempted to fact check that the Obama Administration depleted the stockpile and did nothing to replenish it, or that the budget was cut by the Republican House. Both claims have been fact-checked as true from sources on the left and sources on the right. The fact is that at the end of 2009 the stockpile was depleted and in 2020 we only had about 30 million of the 300 million needed. I feel the truth of the 2010 resupply had its demise in the budget standoffs between the Obama White House and the Tea Party Budget opposition.
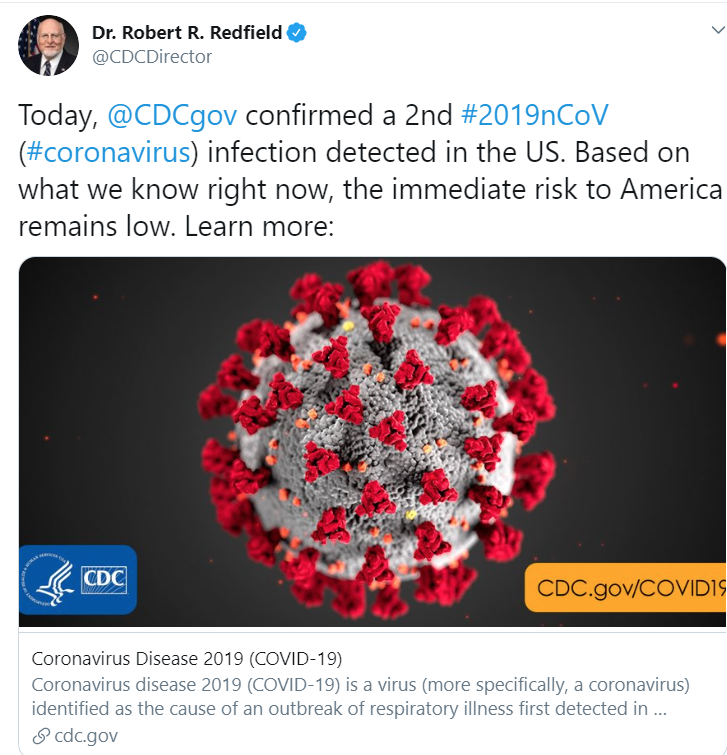
24 Jan, the CDC confirmed the second case in the US and deemed “the immediate risk to America remains low”.
Stage 5: Spread throughout the United States: 26 Jan 2020
On 26 Jan 2020. By the 26th, we now have five cases in the United States, including California and Arizona.
During Stage 5, the USG would support community responses to mitigate illness, suffering, and death. The policy is not always about health; one of the equally essential objectives would be to preserve the critical infrastructure and mitigate the impact on the economy. I say equally, so as not to confuse or suggest the economy is any more or less important than a functioning society.
Responses during Stage 5:
- Deploy pandemic vaccination, if available.
- Continually evaluate the epidemiology and update recommendations on treatment and protective actions
- Provide guidance on judicious use of critical commodities to reduce the likelihood of shortages
Goals:
- Support community response
- preserve critical infrastructure
- Mitigate illness, suffering, and death
- Mitigate impact on the economy and society
Actions
- Maintain overall situational awareness
- evaluate epidemiology; provide guidance on community measures
- Deploy vaccine if available; prioritization guidance
- Sustain critical infrastructure; support health and medical systems, maintain civil order
- Provide guidance on use of key commodities
Policy Decisions
- Federal support of critical infrastructure and availability of key goods and services
- Lifting of travel restrictions
At this point, the Administration has a fundamental policy decision. First, determine whether or not a federal intervention is required to support critical infrastructure and the availability of essential goods. This is also the first look to determine if when travel restrictions previously enacted can be lifted. However, we were slow in adopting travel restrictions, so there were none to lift.
On 28 Jan, Dr. Carter Mecher, Department of Veterans Affairs, sent an email stating that “the projected size of the outbreak already seems hard to believe.”
On 29 Jan, Peter Navarro, in a memo, advised President Trump that the pandemic could cause millions of deaths and trillions in economic losses.
Also on the 29th, the White House formed a coronavirus response task force initially led by Health and Human Services Secretary Alex Azar.
30 Jan the WHO declares that 2019-nCoV outbreak is a public emergency of international concern (PHEIC).
30 Jan the CDC confirms Person-to_Person spread of 2019-nCoV in the United States.
30 Jan, the Trump Administration restricted entry into the US from China. Adding this traveling band is in line with the plan and is designed to limit the transmission. Since then, there has been some evidence that this is an ineffective means. I am sure that this will be addressed in the 2021 Pandemic Strategy.
On the same evening, President Trump held a campaign rally in Iowa and stated “We think we have it very well under control. We have very little problem in this country at this moment — five. … we think it’s going to have a very good ending for it.”
4 Feb the White House directed the CDC to begin shipping a test kit that had nor been cleared or tested by the U.S. Food and Drug Administration (FDA). The test kits began shipping under the issuance of an Emergency Use Authorization from the FDA.
6 Feb the CDC began shipping a CDC-developed laboratory test kit to detect the 2019-nCoV
11 Feb, the virus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was named. The disease in which the virus causes was named coronavirus disease (COVID-19)
Here is a sample of President Trumps messaging regarding COVID-19:
- 2 Feb: “We pretty much shut it down coming in from China. It’s going to be fine.” Discussion with Sean Hannity
- 15 Feb: “the 15 within a couple of days is going to be down to close to zero.” Discussion with Border Patrol Council members.
- 24 Feb: “The Coronavirus is very much under control in the USA… stock market starting to look very good to me!”
- 25 Feb: “I think that’s a problem that’s going to go away. They have studied it. They know very much. In fact, we’re very close to a vaccine.”
- 26 Feb “the 15 cases within a couple of days is going to be close to zero”
Depending on your political leanings, most of the messaging can be grouped into either calming the populace or denying the severity. If you side with calming the population, most of these are fine and would have been better served in mid to late January, so they are about a month off. By the time these were made, the month of February, President Trump should have been advocating for social distancing, suspending unnecessary travel, and other methods to decrease the transmission of the virus.
20 Feb the CDC went to Level 3 Travel Advisory for nonessential travel to South Korea, Taiwan, Japan, and Vietnam.
On the 27th, President Trump created the White House Coronoavirus Task Force. He announced the TF on the 29th and then, on the 31st, declared a public health emergency.
29 Feb the first death from COVID-19 in the US was recorded.
29 Feb issued a proclamation to suspend entry into the US of certain persons that pose a risk of transmitting COVID-19 essentially banning all travel between Iran and the US.
On 6 Mar, in a news conference, President Trump also stated that “anybody that wants a test can get a test”. This type of messaging is very detrimental, it causes confusion. Even today, 13 Apr, that still is not a fact.
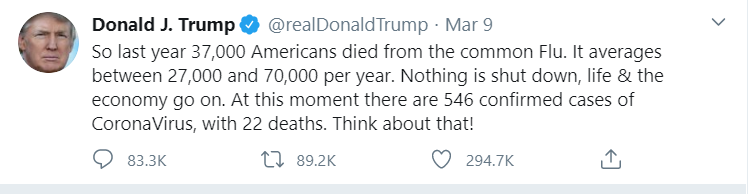
Tweets, like the one above, though factual, is an unwarranted generalization. The problem with the tweet is that it contradicts the need to create the White House Task Force and suggests that there is no need for concern, especially for his base.
11 Mar, the WHO assessed that COVID-19 could be characterized as a pandemic.
12 Mar, further travel restrictions were placed on foreign nationals from most of Europe.
12 Mar Dr. Anthony Fauci testified at a congressional hearing that “it is a failing” that there is not widespread testing available in the United States.
On 13 Mar, President Trump declared a State of emergency and provided guidelines for behavioral modifications, including social distancing. Also, the Emergency Declaration increased the federal government’s effort of mass testing, improve the availability of medical supplies. Further travel restrictions were placed on foreign nationals from most of Europe.
17 Mar, President Trump invoked the Defense Production Act which would allow him to direct industry to produce critical equipment.
Also on 17 Mar, President Trump stated in a news conference that for the next 14 days, “we’re asking everyone to work at home, if possible, postpone unnecessary travel, and limit social gatherings to no more than 10 people.” This was a significant shift in the tone from the White House. Though consistent with the plan, this statement should have been given two months earlier around the 20th of January.
These actions, which help mitigate the spread of the COVID-19, were actions that should have occurred no later than 26 Jan when we entered Stage 5.
As an insult to injury, in the same news conference, President Trump stated “I’ve always known this is real, this is a pandemic. I’ve felt it was a pandemic long before it was called a pandemic.” This message was definitely out of sync with the plan and with his previous messaging. In January, he stated that there were no worries about a pandemic. By late February, he stated that the virus was “very much under control”. Even his actions stated otherwise. He did not activate federal measures to contain the spread until late January.
At this time New York State was becoming the epic center of COVID-19 in the US. On 20 Mar, New York Gov Andrew Cuomo ordered all non-essential businesses to stay at home. Shortly thereafter, Indiana, Louisiana, Ohio, Illinois, and many other states issued similar restrictions.
At this time President Trump began battling with the Governors, even stating that Governor Cuomo “rejected buying recommended 16,000 ventilators in 2015 for the pandemic, for a pandemic, established death panels and lotteries instead. So, he had a chance to buy, in 2015, 16,000 ventilators at a very low price, and he turned it down.” This statement has been determined to be false.
What is interesting is that every tabletop exercise or wargame that I attended, the failure almost always hovered around the coordination between the states and federal government. In some parts it was expectations, others command and control, and lastly authorities. I would have never expected one state to be pitted against another fighting for resources.
The tweet from the 24th has been parroted by numerous Trump supporters as a way to minimize the current state of affairs and ease virus restrictions.
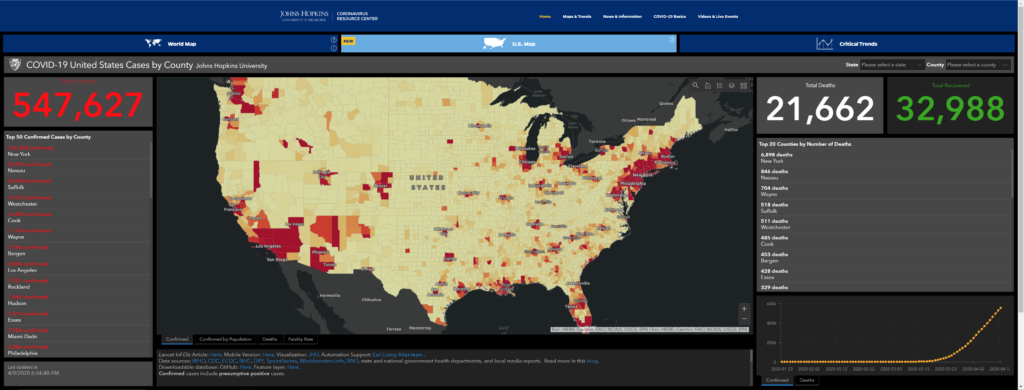
On 26 Mar, the US became to most infected nation on the globe.
29 Mar, the White House extended social distancing guidelines through 30 April and stated that we would be “well on our way to recovery” by 1 June.
Once we transition to Stage 6 and begin Recovery then the steps to normalcy can begin.
From a messaging perspective, all through the National Strategy, it discusses the preparation and deployment of the National Stockpile for domestic use. The notion that the stockpile is for the use of the federal government and not the states is ludicrous.
Activate plans to distribute medical countermeasures, including non-medical equipment and other material, from the Strategic National Stockpile and other distribution centers to federal, state and local authorities.
National Strategy for Pandemic Influenza
November 2005
Stage 6: Recovery and Preparation for Subsequent Waves (WHO Phase 6): unknown
This is a stage that is in our future but is one that is being talked about on a daily basis. The essential items to know is that we need to have the following:
- Rapid diagnostic test
- Treatment/therapy
- Vaccination
There has been news that a rapid diagnostic test is being tested. The President has touted that hydroxychloroquine is a possible treatment, though the scientific community has not confirmed the success.
Analysis
This analysis is based on the government’s reactions compared to the guidelines set up in the implementation plan. However, it should be noted that the implementation plan is not designed to be a checklist of tasks but a strategy that clarifies the roles and responsibilities of governmental and non-governmental entities. I have only discussed Chapters 2 and 3 that describe US Government Planning and Response.
Time will tell of where our successes and failures have been along this journey. The lack of rapid diagnostic testing has been our Achilles heel. Without those, any containment or mitigation strategy is going to suffer. Before we get to a level of normalcy, these must be in place. The lack of synchronization of government response and the President’s messages have negatively influenced the way the population has viewed and reacted to the COVID-19. For the implementation plan to work, the President has to be the mouth-piece and the message on point and consistent. Until we get a rapid diagnostic test, treatment and therapy, and a vaccination, Stage 5 of the Implementation Plan will be a prolonged battle. We may be able to have small pockets of society acting as if they are fully functional, but the US as a whole, we are just at the beginning.